New treatments for chronic myeloid leukaemia (CML), a form of blood cancer, have transformed patient outcomes over the past 20 years. Tyrosine Kinase Inhibitors (TKI) enable CML to be well controlled for most people, and many individuals will live a normal life span. However, early diagnosis and intervention is key to the effective management of this slowly progressing form of leukaemia.
Part of Blood Cancer Awareness month, chronic myeloid leukaemia Awareness Day is on the 22nd September 2020 raising awareness of the need for timely access to diagnosis, treatment and care.
Three Stage Disease
Affecting the white blood cells known as myeloid cells, CML is a disease in which cells that normally would develop into neutrophils, basophils, eosinophils, and monocytes become cancerous. The result of a chromosome relocation, in 95% of cases CML occurs when the BCR gene on chromosome 22 and the ABL1 gene on chromosome 9 swap, creating a new fusion gene - BCR-ABL1. This abnormal gene is located on the new shortened chromosome 22 and is called the Philadelphia chromosome. The Philadelphia chromosome produces an abnormal enzyme (a tyrosine kinase), which is responsible for the abnormal growth pattern of the Ph+ white blood cells in CML.
The disease has three phases. The first or chronic stage of CML is characterised by marked increases in the numbers of normal-appearing white blood cells and sometimes platelets. During the course of the disease, more and more leukaemia cells fill the bone marrow and enter the bloodstream. This period can last from months to years, during which time the disease progresses very slowly. Symptoms, if noticed at all, may be mild, including tiredness, weight loss and a slightly enlarged spleen.
If left untreated, CML will progress to an accelerated phase, during which time treatments are less effective and symptoms worsen – including fatigue and weight loss, as well as pain relating to the enlarged spleen, before moving inevitably to the end stage of the disease, called the blast phase.
In the blast phase, only very immature (blast) leukaemia cells populate the marrow and blood, a sign that the disease has become much worse. Massive enlargement of the spleen is common in the blast phase, as well as fever and weight loss, with the patient at risk of complication such as serious infections and excessive bleeding.
Diagnosing and Treating CML
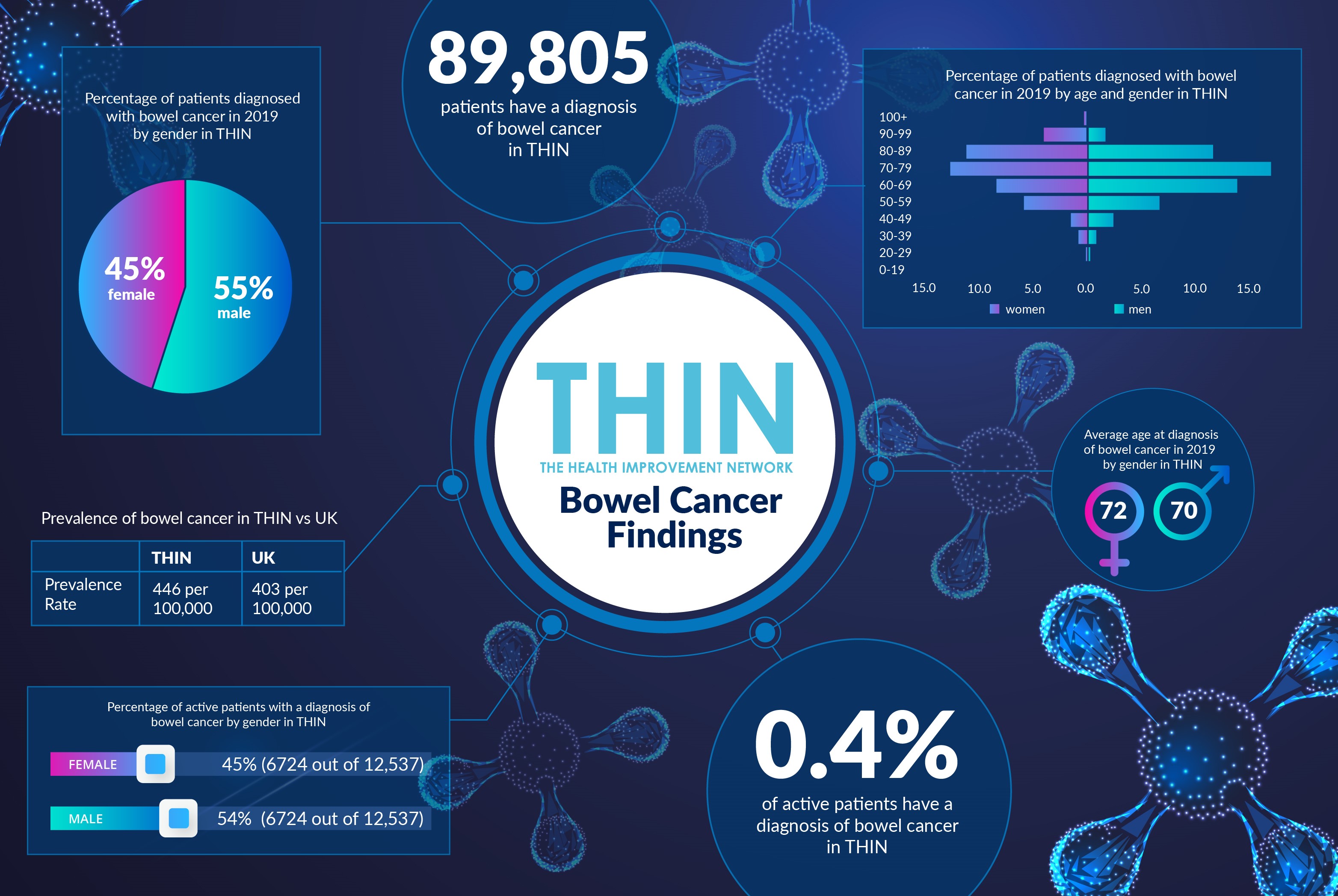
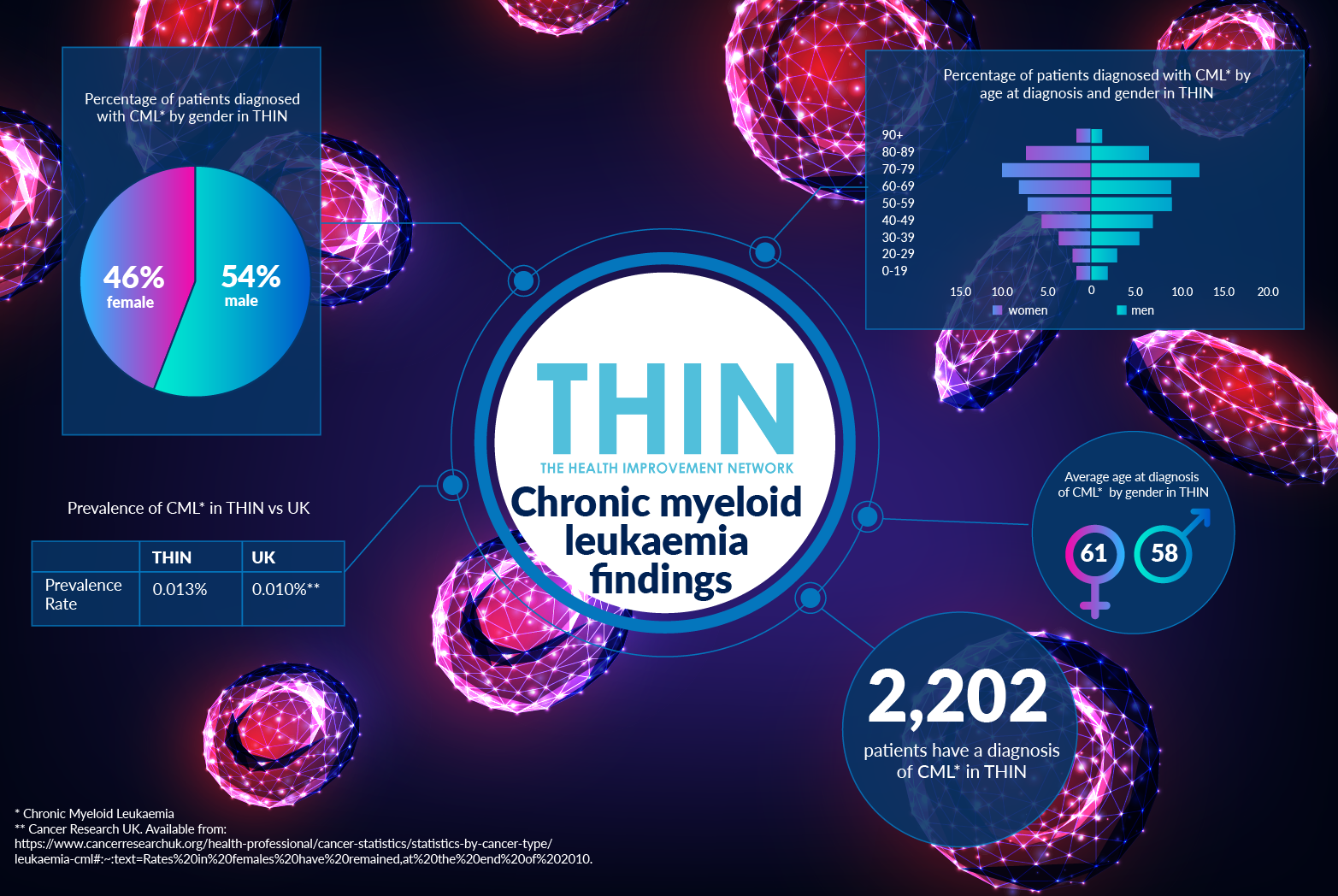
In most cases, there is no obvious cause of CML, indeed exposure to radiation is the only clearly established risk factor. CML is more common in older people and slightly more common in men than women – a fact confirmed by analysis of The Health Improvement Network (THIN®), a Cegedim database.
54% of 2,202 patients with a diagnosis of CML* in THIN® are male. Average age at diagnosis for men is 58, for women is 61. While there are no specific signs or symptoms which would allow a diagnosis of CML to be made, about half of all patients have a swollen spleen. Other issues to consider include anaemia, weakness, tiredness, shortness of breath, light-headedness, palpitations, more frequent and severe infections, fever, malaise and sweats, purpura, nosebleeds, bleeding gums, bleeding and bruising.
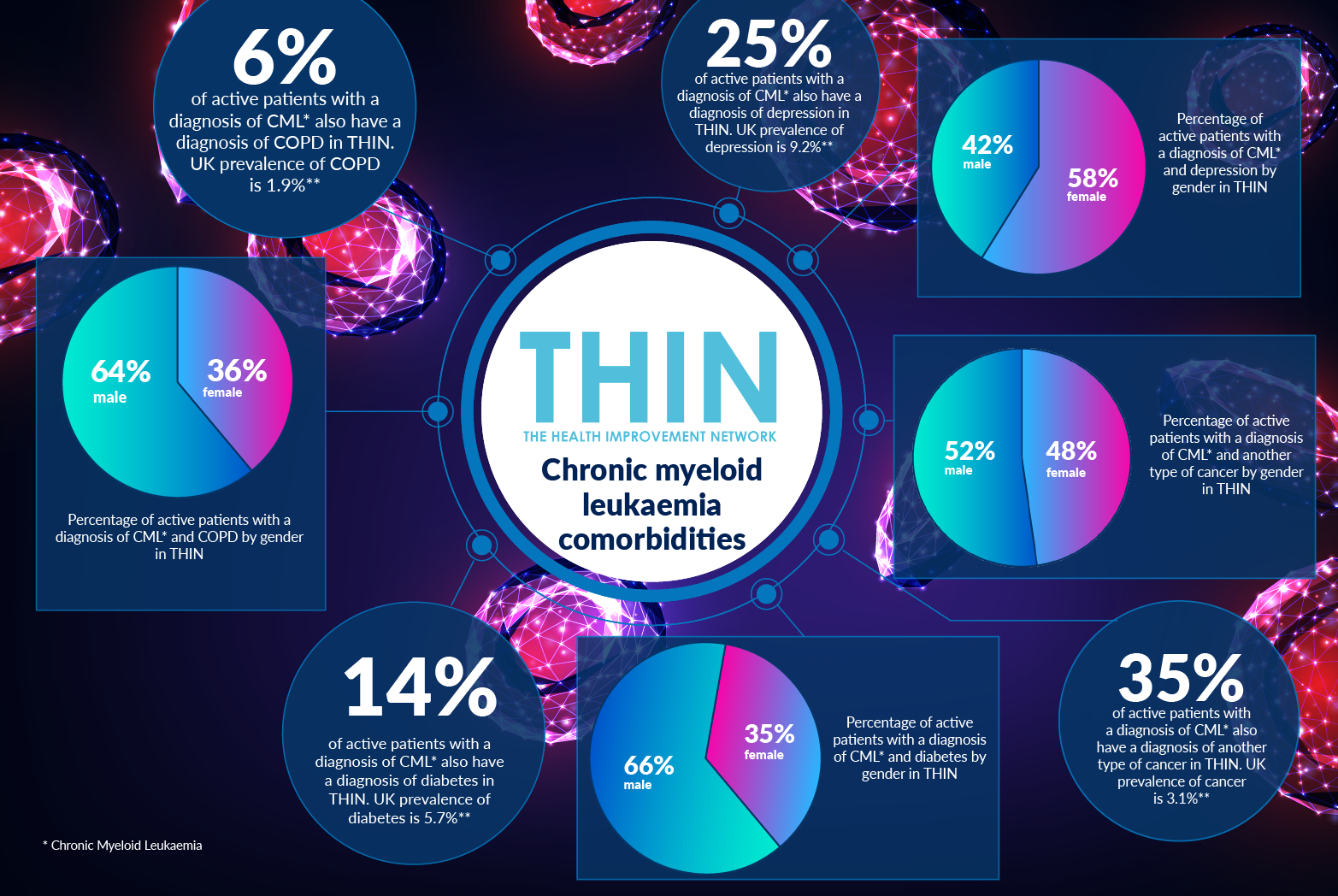
THIN® data also helps us better understand co-morbidities and the different experiences between male and female CML sufferers. One third (35%) of active patients with a diagnosis of CML also have a diagnosis of another type of cancer in THIN®; while just under one sixth (14%) of active patients with a diagnosis of CML also have a diagnosis of diabetes in THIN® – 65% of these patients are male. In addition, 6% of active patients with a diagnosis of CML also have a diagnosis of COPD in THIN®, 64% are male.
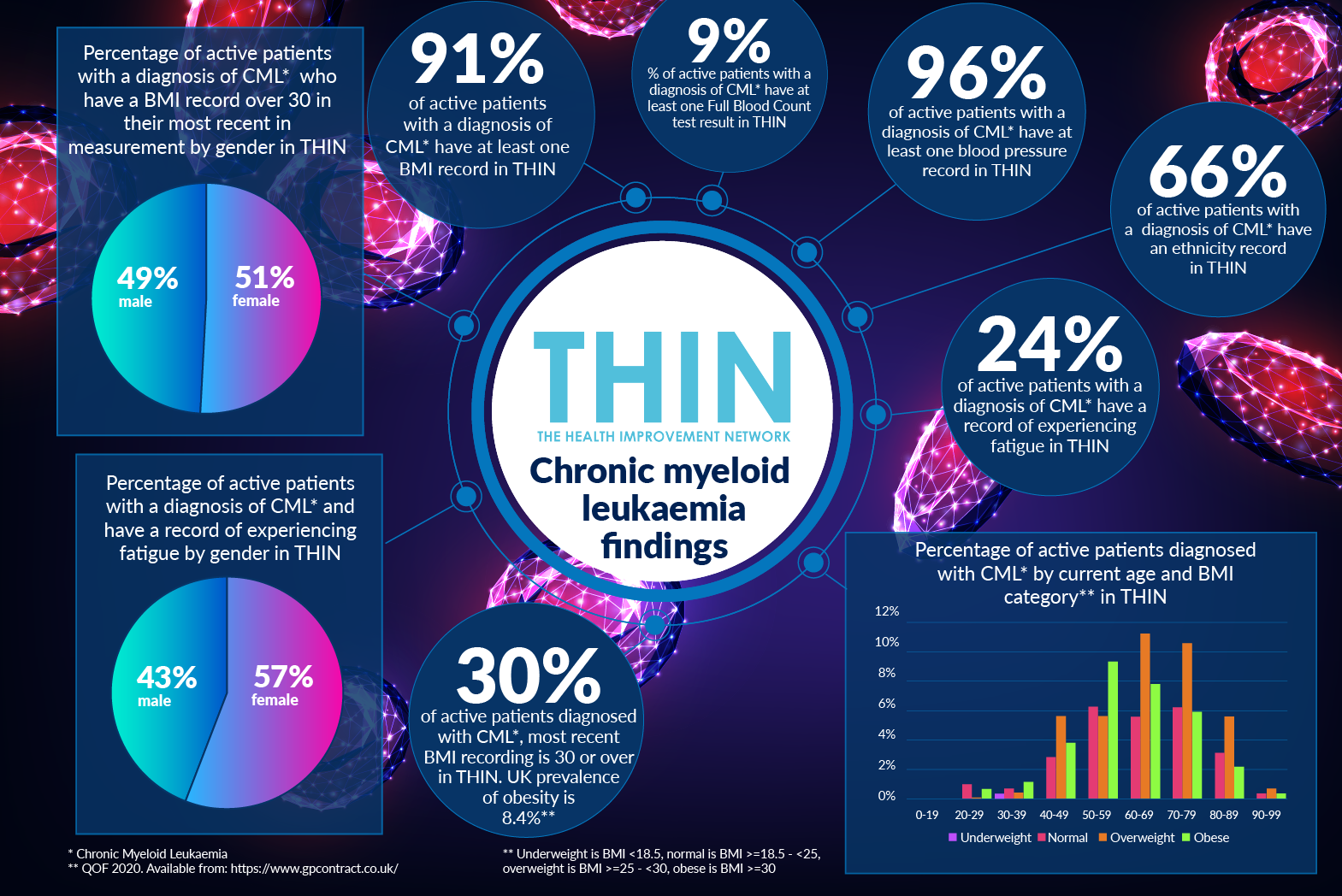
Women are more likely to report fatigue and depression. While 25% of active patients with a diagnosis of CML also have a diagnosis of depression in THIN®, 58% of these are female. Furthermore, 24% of active patients with a diagnosis of CML have a record of experiencing fatigue in THIN® - 57% are female.
THIN® data also reveals a significant proportion of active patients with a diagnosis of CML are obese. 91% of active patients with a diagnosis of CML have at least one BMI record in THIN® and 30% have a BMI recording of 30 or over.
Treating CML
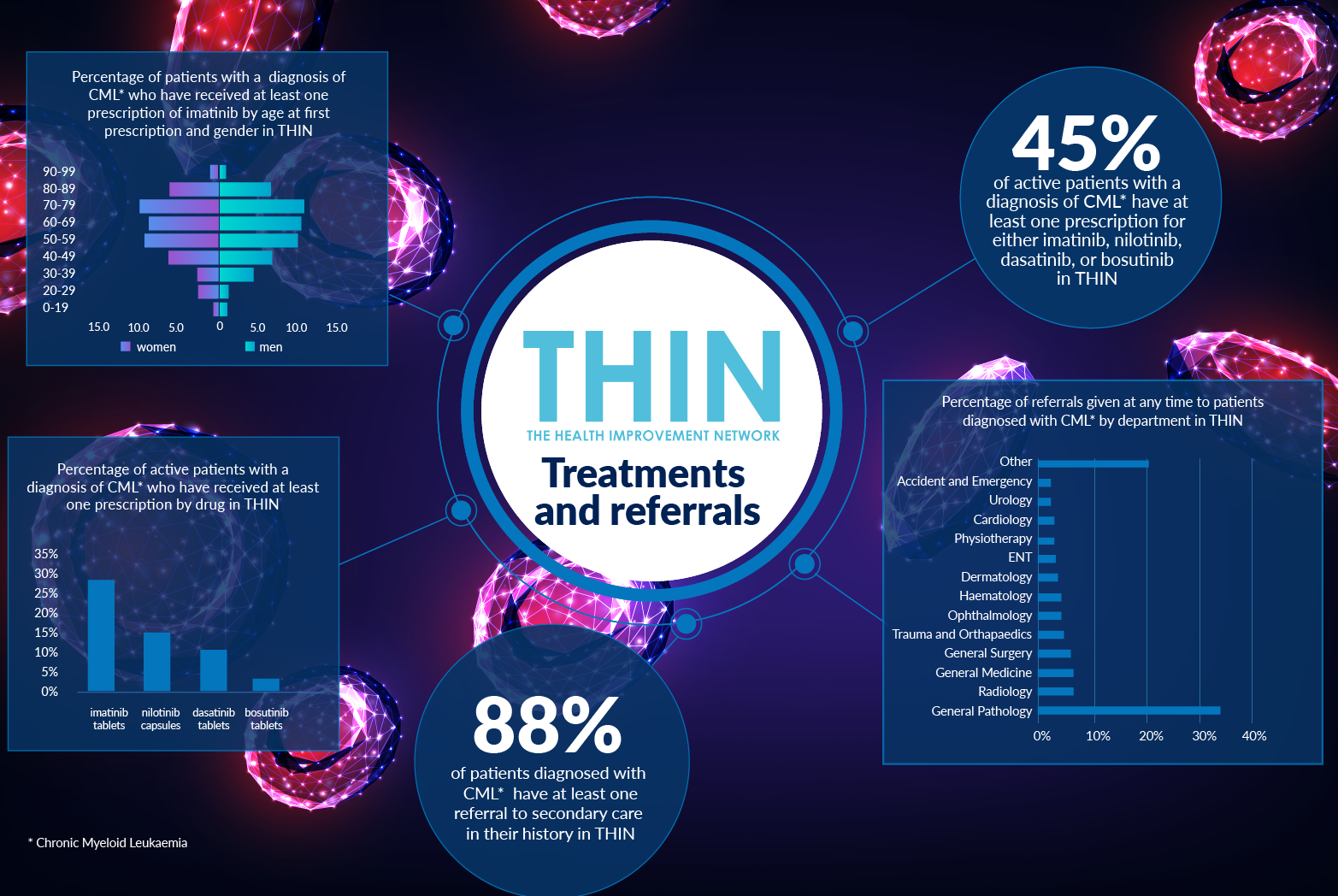
TKIs have become the standard treatment for CML as the drugs block the harmful effect of BCR-ABL. According to THIN® data, 45% of active patients with a diagnosis of CML have at least one prescription from their GP for either imatinib, nilotinib, dasatinib, or bosutinib. A number that would undoubtedly be much higher if THIN® Research Services were used to analyse secondary care prescribing data
According to CML Support, a small but significant patient group respond so well to TKI they are able to stop therapy having achieved a stable molecular response. While TKI therapy has transformed CML, research continues to try to find even better treatment options for patients – hopefully leading to a complete remission or ‘cure’. Work is ongoing to understand which drugs or combinations of drugs could work best for individual patients. Research across many disciplines including gene therapy and immunotherapy will help achieve even better results for CML patients in the future.
This is where population health data can play such a vital role in understanding the progress of CML, through the chronic, accelerated and blast phases. It will help to track the impact of TKI therapy and better understand the impact of co-morbidities on patient experience and outcomes.
About THIN
THIN® is an unobtrusive medical data collection scheme that contains anonymised longitudinal patient records for approximately 6% of the UK population. It is the key driving force behind enabling advancements in patient care and outcomes, with one of the most respected and reliable data sources for anonymised primary care records.