Time for Population Health and Individual Screening to Combine to Address Rising Stroke Events
A stroke can happen to anyone, at anytime and anywhere. Today stroke is the leading cause of disability worldwide and the second leading cause of death, but almost all strokes could be prevented. Being active is one of the ways individuals can reduce their risk of stroke – which is why the World Stroke Organisation was asking people to Join the MoveMent and be a part of the world’s biggest dance chain on #WorldStrokeDay on October 29th.
COVID-19 and Stroke
A stroke affects someone in the UK every ten minutes – that is 100,000 people having strokes every year. This year, however, the impact of stroke has been even more devastating – with a report claiming that thousands of stroke patients have suffered avoidable disability because NHS care was disrupted during the pandemic. In addition to many people who recently experienced a stroke event finding it harder to obtain clot-busting drugs or undergo surgery to remove a blood clot from their brain, rehabilitation services, which are vital to help reduce the impact of a stroke, also stopped working normally as the NHS focused on COVID-19 according to the Stroke Association.
Fear of COVID-19 also played a key role. Three in 10 (29%) of those who had suffered a stroke did not seek emergency help, for example by dialling 999. Similarly, while half of stroke survivors had sessions of therapy cancelled, 56% did not feel safe to attend a scheduled appointment. Recent figures suggest that 52% more people than usual died of a stroke at home during the pandemic.
In addition, there is a growing suggestion that brain complications, including stroke and psychosis, have been linked to COVID-19. This study follows early observations into the pandemic in the US that people as young as 30 are experiencing strokes, even when their COVID-19 symptoms were mild.
It is also becoming clear that hypertension is associated with increased composite poor outcome, including mortality, severe COVID-19, ARDS, need for ICU care and disease progression in patients with COVID-19.
Stroke Comorbidities
Understanding the comorbidities of stroke is vital in improving targeted health care and prevention – which is where The Health Improvement Network (THIN®), a Cegedim database, is providing vital insight to support both clinicians and population health planning.
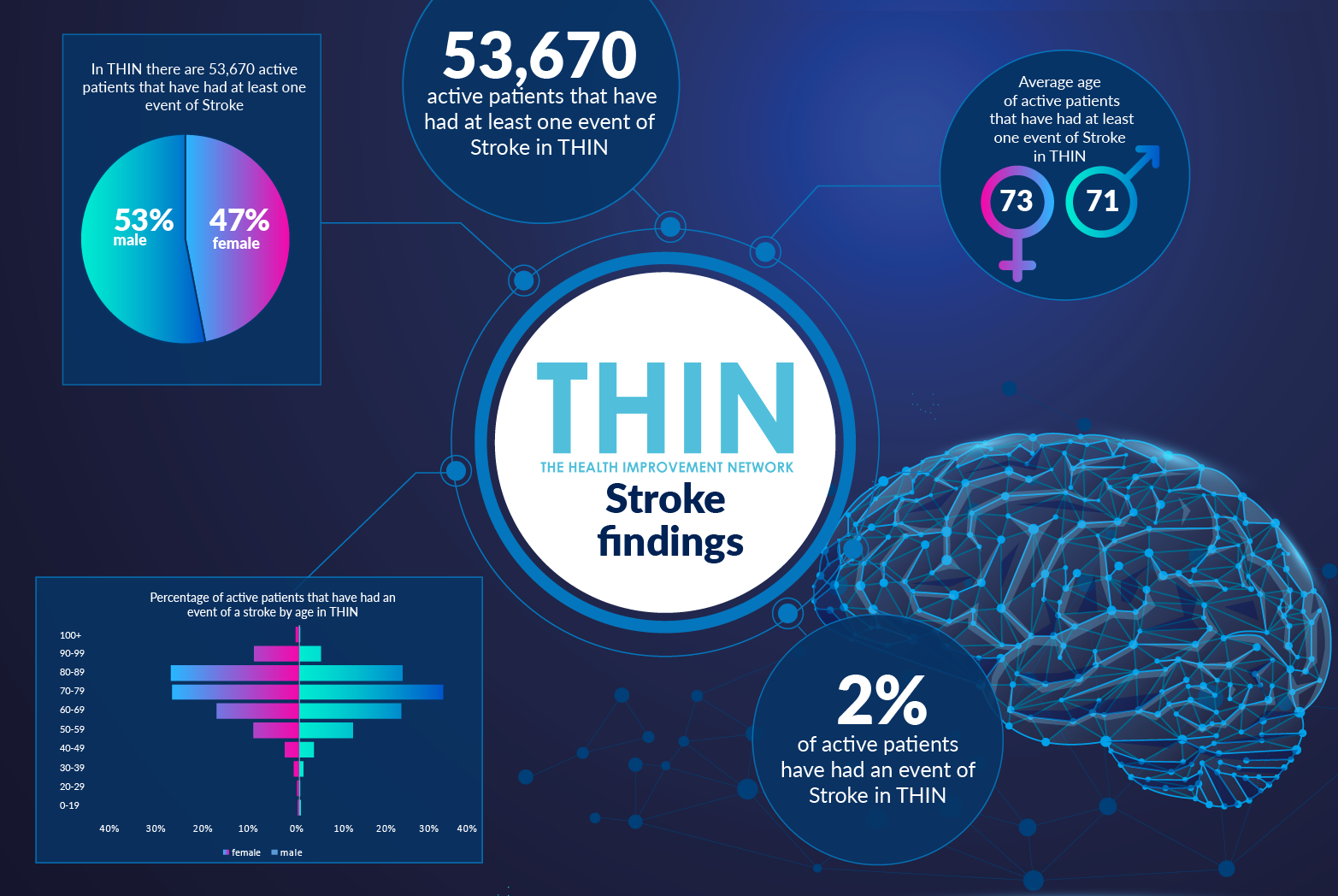
In THIN® there are 53,670 active patients that have had at least one event of stroke – 2% of active patients. Looking at patients that have had a stroke event, the majority (91%) of patients have had at least one or two events. Just 1% of the active patients have experienced more than 6 stroke events. Women make up 47% of the active patients within THIN® that have experienced at least one event of stroke – the average age of active patients is 71 for men and 73 for women.
Given the growing evidence of hypertension and COVID-19, it is also revealing that 57% of active patients in THIN® that have experienced stroke also have a diagnosis of hypertension. In addition, 27% of active patients in THIN® that have experienced stroke also have a diagnosis of diabetes; 23% also have a diagnosis of chronic kidney disease (CKD) and 20% have a diagnosis of coronary heart disease (CHD).
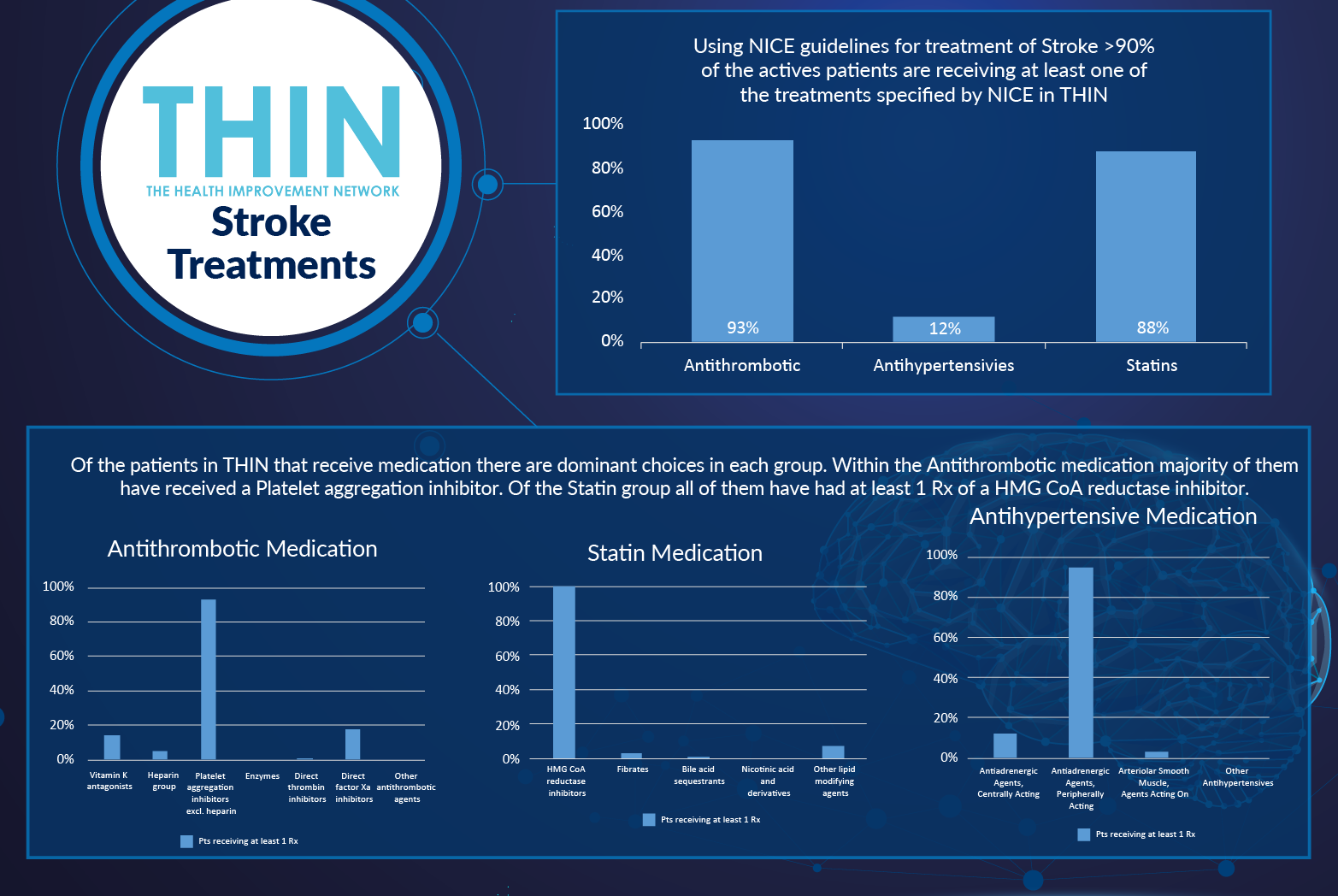
Treatment for stroke is well established under NICE guidelines. THIN® analysis confirms that over 90% of active patients are receiving at least one of the treatments specified by NICE: Antithrombotic medication (93%), Antihypertensive medication (12%) and Statins (88%). Of the patients that receive medication there are dominant choices in each group. Within the Antithrombotic medication, the majority have received a Platelet aggregation inhibitor. Of the Statin group, all have had at least 1 Rx of a HMG CoA reductase inhibitor.

Population Health
However, while treatment pathways are well established, global initiatives to prevent strokes are not working. Improving diet and increasing exercise are vital steps in preventing strokes, alongside reducing hypertension. Yet while adult lifetime risk of stroke was one in six less than a decade ago, in 2020 it is one in four – and that is without factoring in the additional risks created by COVID-19.
So what is going wrong? A recent report from the World Stroke Organisation (WSO) confirms that 80% of strokes happen to people who are not categorised as high-risk and calls for a change in approach – namely, moving away from the widely adopted approach of individual clinical risk factor screening towards investment in primary prevention at population level. This would see governments prioritising alcohol and tobacco control measures, reducing consumption of salt and trans fats from processed food and addressing sedentary lifestyles.
In tandem with the World Heart Federation, the WSO insists that identifying and labelling individuals as low risk reduces their motivation to take action on smoking, physical inactivity, diet and alcohol. Stating, “By placing all our bets on identifying and treating diseases of the circulatory system, we are missing the opportunity to intervene on their shared causes much earlier in the prevention timeline where the costs are lowest. The benefit-cost ratio is 10.9 for every dollar spent on population-wide primary prevention. While there is a place for screening and management of clinical risk factors, our strong recommendation is that it should be complementary to population-based strategies, not the other way around.”
This is where THIN® is so valuable – supporting not only clinicians in identifying those at high risk but also underpinning population health planning to identify otherwise low risk individuals who need to make radical changes to diet and exercise to minimise their risk.
About THIN®
THIN® is an unobtrusive medical data collection scheme that contains anonymised longitudinal patient records for approximately 6% of the UK population. It is the key driving force behind enabling advancements in patient care and outcomes, with one of the most respected and reliable data sources for anonymised primary care records.